In addition, the experience of radiographers performing a screening examination in women with an IMD is included in this study. More information about the study can be found here. Here we present important issues for best practice performing a screening examination in women with an IMD.
ICD, pacemaker, hearth rhythm monitor, porth-a-cath
- Women with an ICD, pacemaker, hearth rhythm monitor or porth-a-cath can participate in breast cancer screening.
- We advise that women do not participate in the screening programme until 6 months after implantation of every type of medical device, to give the breast enough recovery time after implantation.
- It’s always important to inform a woman before and after the screening examination about the procedure. For women with an IMD careful explanation about the procedure can be highly relevant to reduce anxiety.
S-ICD
- We advise that women with a subcutaneaous ICD (S-ICD) do not participate in an organized screening programme outside a hospital setting.
- Most women with a S-ICD will be aware of their type of ICD. The location of the S-ICD is different compared to the conventional ICD. The S-ICD generator is placed under the skin on the left side of the chest at the height of the 5th/6th rib (see Figure below). The electrode is placed under the skin along the sternum, close underneath the mamma to the generator.
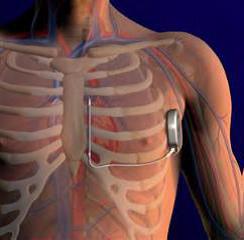
Figure: The location of the subcutaneaous ICD (S-ICD)
During the screening examination
- Uniformity and reproducibility are essential for high technical image quality. Therefore, work according to standard positioning technique and at least make sure that the breast is fixed fairly solidly in place. It is important to project as much breast tissue as possible, to project a sufficiently wide musculus pectoralis, and to compress (part of) the area where the device is located if necessary.
- If positioning technique and physical-technical image quality is less than the MLO-view of the breast without IMD, take an additional MLO-image of the caudal part of the breast (lower bucky position)
- When compression force is low, we recommend to give a breathing command during the examination, thereby reducing the chance on a blurred image.
- Image processing could be influenced by an IMD, which could lead to insufficient image quality. At first, radiographers should take an image of the breast without IMD with automatic exposure. Then, use manually exposure in the breast with IMD, with the kV and mAs values of the first image
- Usually, the compression force is higher in women with large mammae. Therefore, we advise to project the breast with IMD at the MLO-view in two parts, in order to avoid large compression on the IMD.